High uric acid may point to gout or kidney issues; it is not a diagnosis on its own.
Educational guide only — not medical advice. Always review results with a qualified clinician.
7 min read
··Last updated
NNoryaAI
High uric acid: what your blood test result means
Uric acid is a natural waste product formed when the body breaks down purines—substances found in certain foods and also produced by the body during normal cell turnover. Under healthy conditions, uric acid dissolves in the blood, passes through the kidneys, and is excreted in urine. However, when the body produces too much uric acid or the kidneys cannot excrete enough, blood levels rise—a condition called hyperuricemia.
Elevated uric acid is best known for causing gout, a painful form of inflammatory arthritis, but it is also linked to kidney stones, chronic kidney disease, hypertension, and cardiovascular risk. Conversely, very low uric acid levels are uncommon but can occur in certain liver or kidney disorders. Understanding your uric acid level helps you and your doctor assess metabolic health and take preventive measures.
This guide is educational and does not replace medical advice. Always discuss your lab results with a qualified healthcare professional.
What is uric acid and how is it produced?
Purines are nitrogen-containing compounds found in every cell in the body and in many foods. When cells die and their DNA is recycled, or when you eat purine-rich foods, the purines are metabolized by the enzyme xanthine oxidase into uric acid. In most mammals, uric acid is further broken down into a more soluble compound called allantoin by the enzyme uricase, but humans lack this enzyme due to a mutation that occurred millions of years ago. As a result, uric acid is the final breakdown product of purine metabolism in humans and must be excreted by the kidneys and, to a lesser extent, the gut.
Approximately two-thirds of uric acid is eliminated by the kidneys, while the remaining one-third is excreted via the gastrointestinal tract. The kidneys filter uric acid from the blood, reabsorb most of it in the proximal tubule, and then secrete a portion back into the tubular fluid for excretion. This complex handling means that kidney function has a profound impact on uric acid levels. Transporters such as URAT1 and GLUT9 play key roles and are targets for some uric-acid-lowering medications.
Interestingly, uric acid also functions as an antioxidant in the blood, accounting for roughly half of the antioxidant capacity of plasma. Some researchers believe this antioxidant role may explain why the uricase gene was lost during human evolution—higher uric acid levels may have conferred a survival advantage. However, the benefits are limited, and chronically elevated levels clearly cause harm.
Normal uric acid ranges
Group
Normal range (mg/dL)
Normal range (µmol/L)
Men
3.4 – 7.0
200 – 420
Women
2.4 – 6.0
140 – 360
Women generally have lower uric acid levels than men because estrogen promotes uric acid excretion by the kidneys. After menopause, women's uric acid levels tend to rise and approach those of men. Children typically have lower levels than adults.
The solubility limit of uric acid in body fluids at normal body temperature is approximately 6.8 mg/dL. Above this concentration, monosodium urate crystals can form in joints and tissues, potentially leading to gout. For patients with gout, treatment guidelines recommend a target uric acid level below 6.0 mg/dL to dissolve existing crystals and prevent future attacks.
Causes of high uric acid (hyperuricemia)
Hyperuricemia results from either overproduction of uric acid, underexcretion by the kidneys, or a combination of both. Underexcretion accounts for about 90% of cases:
Dietary and lifestyle factors:
Purine-rich diet – organ meats (liver, kidney, sweetbreads), red meat, shellfish (shrimp, lobster, mussels), and certain fish (anchovies, sardines, herring) are high in purines.
Alcohol – beer is particularly problematic because it contains guanosine, a purine. Alcohol also increases uric acid production while reducing renal excretion. Spirits and wine have a smaller but still significant effect.
Fructose and sugar-sweetened beverages – fructose metabolism generates purines as a byproduct, directly increasing uric acid production. High-fructose corn syrup is a major contributor.
Obesity – excess body fat increases purine production and reduces renal uric acid clearance.
Medical conditions:
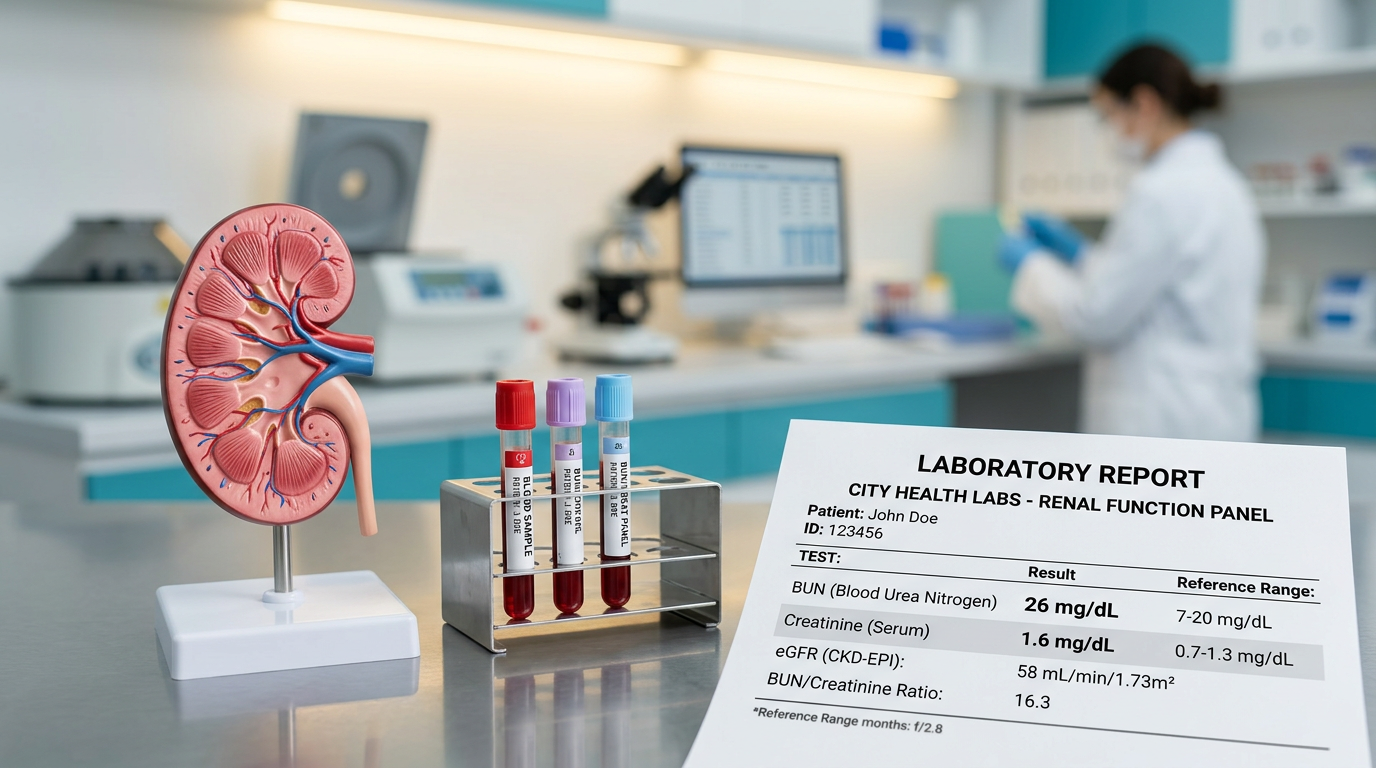
Chronic kidney disease – impaired kidney function reduces uric acid excretion. For more on kidney markers, see our guide on creatinine and eGFR.
Myeloproliferative and lymphoproliferative disorders – conditions with rapid cell turnover (leukemia, lymphoma, psoriasis) produce excess purines.
Hypothyroidism, lead toxicity, and pre-eclampsia can also elevate uric acid.
Medications: Thiazide and loop diuretics, low-dose aspirin, cyclosporine, pyrazinamide, and ethambutol reduce renal uric acid excretion. Chemotherapy drugs can cause tumor lysis syndrome with dramatic uric acid spikes.
Uric acid and gout
Gout is an inflammatory arthritis caused by the deposition of monosodium urate (MSU) crystals in joints and surrounding tissues. It is the most common inflammatory arthritis in men and increasingly prevalent worldwide, partly due to rising rates of obesity, metabolic syndrome, and dietary changes.
The classic gout attack presents as sudden, excruciating pain, swelling, redness, and warmth in a single joint—most commonly the base of the big toe (podagra). Attacks often begin at night and peak within 12–24 hours. Without treatment, an attack typically resolves in 1–2 weeks but tends to recur and may involve more joints over time.
Not everyone with hyperuricemia develops gout. Population studies show that only about 20–25% of people with uric acid above 9 mg/dL develop gout over a 5-year period. However, the risk increases sharply with higher levels and longer duration of hyperuricemia. Chronic untreated gout can lead to tophi (hard deposits of urate crystals under the skin), joint erosion, and permanent joint damage.
Management of gout involves treating acute flares with NSAIDs, colchicine, or corticosteroids, and long-term urate-lowering therapy (usually allopurinol or febuxostat) for patients with recurrent attacks or complications.
Uric acid and kidney stones
Uric acid kidney stones account for approximately 10% of all kidney stones in developed countries and up to 40% in some Middle Eastern and Mediterranean populations. They form when urine is persistently acidic (low pH), concentrated, and contains excess uric acid.
Unlike calcium-based kidney stones, uric acid stones are radiolucent—they do not show up on standard X-rays and require CT scan or ultrasound for detection. Risk factors include chronic diarrhea (which causes bicarbonate loss and acidic urine), type 2 diabetes (associated with low urine pH), obesity, high-purine diets, and dehydration.
Prevention of uric acid stones focuses on urinary alkalinization (raising urine pH to 6.0–6.5 with potassium citrate), adequate hydration (at least 2–2.5 liters of fluid daily), dietary purine restriction, and, when necessary, allopurinol to reduce uric acid production. Unlike calcium stones, uric acid stones can often be dissolved with medical therapy alone, avoiding the need for surgical intervention.
Dietary recommendations for managing uric acid
Diet plays a meaningful role in uric acid management, though it typically accounts for only about a 1–2 mg/dL change in serum uric acid. Nevertheless, dietary modifications are an important complement to medication when needed:
Foods to limit or avoid:
Organ meats – liver, kidney, sweetbreads are extremely high in purines.
Certain seafood – anchovies, sardines, herring, mussels, scallops, and shrimp.
Red meat – beef, lamb, and pork in large quantities.
Alcohol – especially beer and spirits.
Sugar-sweetened beverages and high-fructose foods – sodas, fruit juices, candy.
Foods that may help:
Low-fat dairy products – milk and yogurt have been shown to lower uric acid levels.
Cherries and cherry extract – several studies suggest they reduce gout flare frequency.
Coffee – regular coffee consumption is associated with lower uric acid levels.
Vitamin C – modest uricosuric effect at doses of 500 mg/day or more.
Plenty of water – adequate hydration helps the kidneys excrete uric acid.
Vegetable purines (from spinach, mushrooms, asparagus) do not appear to increase gout risk and need not be restricted. A balanced diet emphasizing whole grains, vegetables, fruits, and lean proteins is recommended.
Medications for high uric acid
Medications to lower uric acid are primarily used in patients with gout, uric acid kidney stones, or very high uric acid levels. They fall into two main categories:
Xanthine oxidase inhibitors (reduce production):
Allopurinol – the most widely used urate-lowering drug. Started at a low dose and titrated to achieve a target serum uric acid below 6.0 mg/dL. Generally well tolerated; rare but serious hypersensitivity reactions are associated with the HLA-B*5801 allele, which should be tested in high-risk populations (Southeast Asian, African American).
Febuxostat – a selective xanthine oxidase inhibitor alternative for patients who cannot tolerate allopurinol. More potent but carries a cardiovascular safety warning.
Uricosuric agents (increase excretion):
Probenecid – increases renal uric acid excretion. Requires adequate kidney function and hydration; contraindicated in patients with a history of uric acid kidney stones.
Lesinurad – a newer URAT1 inhibitor used in combination with a xanthine oxidase inhibitor.
When initiating urate-lowering therapy, gout flares can paradoxically increase during the first months as crystal deposits dissolve. Prophylactic colchicine or low-dose NSAIDs are often prescribed during this transition period. Treatment is typically lifelong.
When to see a doctor
Consult your doctor about your uric acid levels in the following situations:
Your uric acid is above 7.0 mg/dL (men) or 6.0 mg/dL (women) on repeated testing.
You have symptoms of gout: sudden, severe joint pain with swelling, redness, and warmth, especially in the big toe.
You have a history of kidney stones, especially if they are uric acid stones.
You are taking medications known to raise uric acid (diuretics, low-dose aspirin).
You have chronic kidney disease with elevated uric acid, which may accelerate kidney damage.
You notice tophi—firm, chalky nodules under the skin near joints or on the ears.
Asymptomatic hyperuricemia (elevated uric acid without gout or stones) is common and does not always require treatment. However, it warrants lifestyle modifications and monitoring, especially when accompanied by other metabolic risk factors such as obesity, diabetes, or hypertension.
How Norya helps you understand your uric acid results
Interpreting uric acid in the context of your complete blood panel can be complex. Norya makes it simple: upload your blood test results and receive a clear, structured health summary within minutes. Norya evaluates your uric acid alongside kidney function markers, glucose, lipids, and inflammation indicators to give you a comprehensive metabolic picture.
The report flags abnormal values, explains their significance in everyday language, and prepares you with the right questions for your doctor visit. Start your free analysis with Norya.
Disclaimer
This guide is for informational purposes only and does not replace medical advice or diagnosis. Always discuss your results with a healthcare professional. Start analysis with Norya
Trust & review
How this guide should be used
This article is educational and should be reviewed alongside our medical review, methodology, and transparency pages. Use it to prepare for a clinician conversation, not as a diagnosis.