Understand what T3 and T4 mean, how they relate to TSH, and what abnormal thyroid hormone results may suggest.
Educational guide only — not medical advice. Always review results with a qualified clinician.
8 min read
··Last updated
NNoryaAI
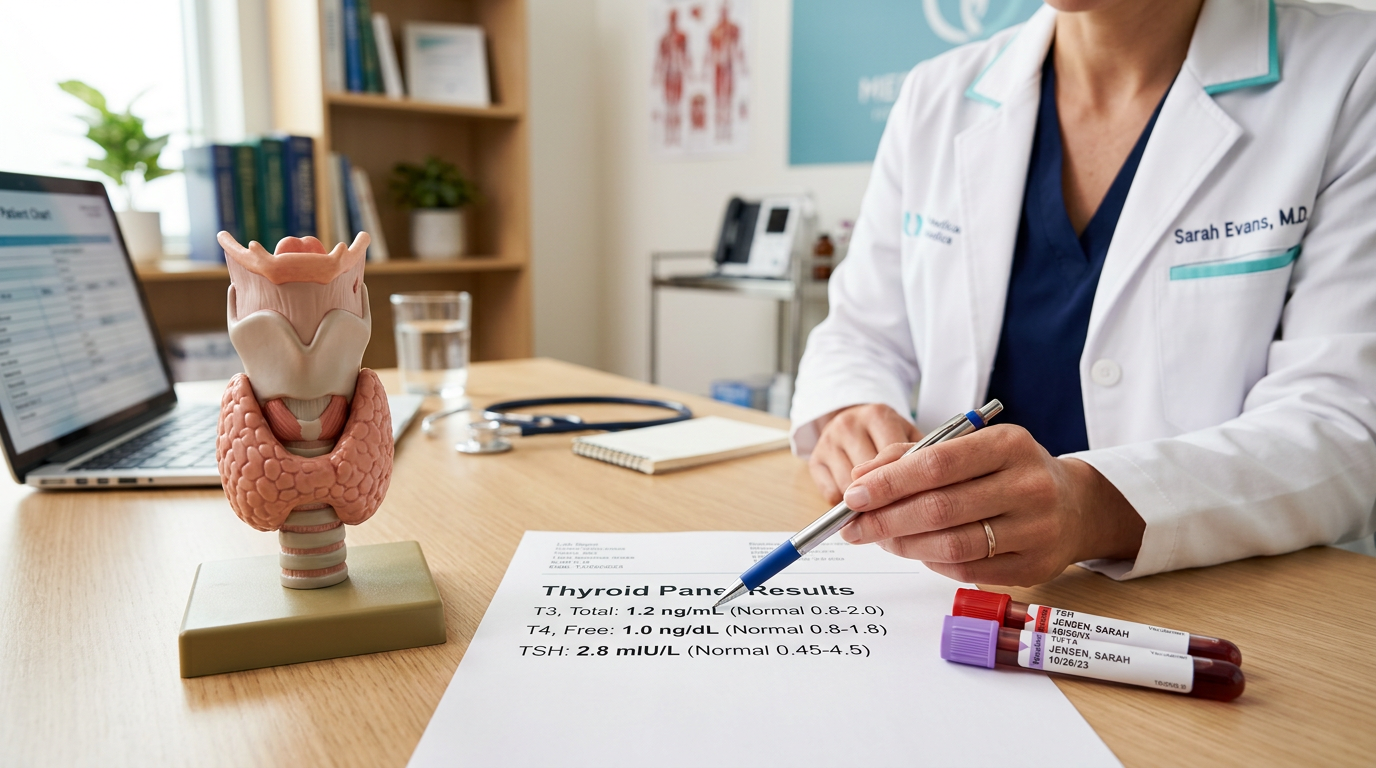
T3 & T4: Understanding Your Thyroid Hormones
When you see T3 and T4 on your blood test report, the first question is often: what do these hormones do, and are my results normal? Triiodothyronine (T3) and thyroxine (T4) are the primary hormones produced by the thyroid gland. They play a central role in regulating metabolism, energy production, growth, and development. Because they influence virtually every cell in the body, abnormal levels can manifest as symptoms ranging from fatigue and weight changes to heart-rate disturbances and hair loss.
This guide explains what T3 and T4 are, how they differ, what the reference ranges mean, and what can cause abnormal results. Our goal is not to diagnose but to help you understand your results so you can have a more productive conversation with your doctor.
What are T3 and T4?
T3 (triiodothyronine) and T4 (thyroxine) are hormones produced by the butterfly-shaped thyroid gland in the neck. T4 is the thyroid's primary secretory product and accounts for roughly 80 % of circulating thyroid hormone. However, T4 has relatively low biological activity; it is converted in peripheral tissues—mainly the liver and kidneys—into the more potent T3 by enzymatic removal of one iodine atom. T3 is the principal effector hormone that directly accelerates cellular metabolism.
Together, these hormones regulate protein synthesis, oxygen consumption, cardiac output, gut motility, and brain development. During childhood they are critical for growth and neurological maturation, while in adults they maintain basal metabolic rate. When thyroid hormone levels are too high or too low, virtually every organ system in the body can be affected.
T3 vs T4: what is the difference?
T4 is the thyroid's main product and circulates at higher concentrations in the blood. Its half-life is approximately 6–7 days, making blood levels relatively stable throughout the day and a reliable laboratory marker. T3 is 3–5 times more biologically potent than T4 but circulates in much smaller quantities; its half-life is only about 1 day. Most circulating T3 is produced by conversion from T4 in peripheral tissues rather than by direct thyroid secretion.
In clinical practice, Free T4 and TSH are usually measured first. T3 is added when T4 is normal but TSH is suppressed, or when hyperthyroidism is clinically suspected, because some patients have isolated T3 elevation (T3 thyrotoxicosis). Evaluating both hormones together provides the most complete picture of thyroid function.
Free vs total hormones
The majority of T3 and T4 circulating in the blood is bound to carrier proteins—primarily thyroxine-binding globulin (TBG). The bound fraction is biologically inactive; only the free (unbound) fraction can enter cells and exert metabolic effects. Total T4 and Total T3 measure the sum of bound and free forms, while Free T4 (FT4) and Free T3 (FT3) measure only the active unbound portion.
Conditions such as pregnancy, estrogen therapy, liver disease, or genetic TBG variants can alter carrier-protein levels, shifting total values without necessarily changing the free hormone concentration. For this reason, modern thyroid assessment relies primarily on free hormone measurements, which more accurately reflect the biologically active hormone available to tissues.
T3 and T4 reference ranges
The table below shows commonly accepted reference ranges for thyroid hormones in adults. Because methodologies vary between laboratories, slight differences are normal; always refer to the reference range printed on your own report.
Test
Normal Range
Free T4
0.8 – 1.8 ng/dL
Free T3
2.3 – 4.2 pg/mL
Total T4
4.5 – 12.5 μg/dL
Total T3
80 – 200 ng/dL
TSH
0.4 – 4.0 mIU/L
These values apply to the general adult population. Pregnancy, age, medications, and chronic illnesses can shift reference ranges. Always interpret your results alongside your own laboratory's reference range and clinical context.
Causes of high T3 and T4 (hyperthyroidism)
When T3 and/or T4 levels are above the reference range, the condition is called hyperthyroidism. The most common causes include: Graves' disease (autoantibodies stimulate the thyroid to overproduce hormone), toxic nodular goiter (autonomously functioning thyroid nodules), thyroiditis (inflammation of the gland that releases stored hormone into the bloodstream), and excess thyroid medication.
In hyperthyroidism the metabolic rate increases, potentially causing palpitations, weight loss, excessive sweating, tremor, nervousness, and diarrhea. In some patients only T3 is elevated (T3 thyrotoxicosis) while T4 remains normal. Diagnosis requires combining clinical signs with laboratory findings and, in some cases, thyroid imaging.
Causes of low T3 and T4 (hypothyroidism)
When T3 and/or T4 levels fall below the reference range, the condition is called hypothyroidism. The most common cause worldwide is Hashimoto's thyroiditis, an autoimmune condition in which the immune system attacks thyroid tissue, gradually reducing hormone production. Other causes include iodine deficiency, pituitary gland disorders (secondary hypothyroidism), post-surgical or post-radioactive-iodine states, and certain medications such as lithium and amiodarone.
In hypothyroidism the metabolic rate slows, leading to fatigue, weight gain, cold intolerance, constipation, dry skin, hair loss, facial puffiness, depressed mood, memory difficulties, and bradycardia. Diagnosis is typically based on elevated TSH combined with low Free T4; treatment usually involves synthetic thyroxine (levothyroxine) replacement.
The TSH–T3–T4 feedback loop
TSH (thyroid-stimulating hormone) is secreted by the pituitary gland and tells the thyroid how much T3 and T4 to produce. When circulating thyroid hormone levels drop, the pituitary releases more TSH to stimulate the thyroid (negative feedback); when hormone levels are adequate, TSH is suppressed. This dynamic equilibrium keeps the metabolic rate within a narrow range.
Clinically, TSH is the most sensitive screening test: in early hypothyroidism, TSH begins to rise before T4 falls below normal (subclinical hypothyroidism); in early hyperthyroidism, TSH is suppressed before T4 is frankly elevated. Doctors therefore usually check TSH first and add Free T4 and T3 as needed. The generally accepted normal range for TSH is 0.4–4.0 mIU/L, although individual targets may vary with age and clinical context.
Symptoms of thyroid hormone imbalance
Hyperthyroid symptoms: palpitations, unintended weight loss, excessive sweating, heat intolerance, tremor (especially of the hands), restlessness, insomnia, frequent bowel movements or diarrhea, muscle weakness, and menstrual irregularities in women. In Graves' disease, eye abnormalities (exophthalmos) may also be present.
Hypothyroid symptoms: fatigue, weight gain, cold intolerance, constipation, dry skin, hair and eyebrow thinning, edema (particularly around the face and eyes), depressed mood, memory problems, and bradycardia. Because symptoms develop gradually, patients may not notice them for months or even years.
In both conditions, symptoms are non-specific and cannot alone confirm a diagnosis. Laboratory tests and clinical evaluation must be considered together.
When should you see a doctor?
If any of your T3, T4, or TSH values fall outside the reference range, consulting a doctor is recommended. Seek medical attention especially if you notice unexplained weight changes, persistent fatigue, palpitations, tremor, hair loss, constipation or diarrhea, mood disturbances, or a visible swelling in the neck.
Early detection of thyroid disorders improves treatment outcomes. Individuals with a family history of thyroid disease, those with autoimmune conditions, women who are pregnant or planning pregnancy, and anyone who has received radiation therapy to the neck area should undergo regular thyroid screening. Even in subclinical cases, your doctor may recommend a monitoring plan.
How Norya helps you understand your thyroid results
At Norya we don't diagnose—we make it easier for you to understand your blood test and prepare for your doctor's visit. You can upload your report and receive a clear, structured summary that explains your T3, T4, and TSH values in plain language alongside reference ranges. This summary helps you walk into your appointment better prepared.
Ready in just a few minutes, the report highlights which values are within range and which fall outside, helping you organize your questions before you see your doctor. For options and pricing, visit our pricing page.
Disclaimer
This guide is for informational purposes only and does not replace medical advice or diagnosis. Always discuss your results with a healthcare professional. Start analysis with Norya
Trust & review
How this guide should be used
This article is educational and should be reviewed alongside our medical review, methodology, and transparency pages. Use it to prepare for a clinician conversation, not as a diagnosis.